Dear email subscribers: this post may be too long for an email, so click on the title to read the online version!
Rintrah Radagast posted a very important article yesterday. It shows us a potential explanation of why excess mortality is related to COVID boosters, why the association of Covid vaccines with mortality strengthens as time goes on instead of declining, and why boosted people take the longest to clear Covid-19.
Check Rintrah’s article out. It is brilliant and very disturbing.
Rintrah is discussing a very important scientific study that answers a question: what exactly are those antibodies that Covid-boosted people are developing?
This study answering that question is here:
Rintrah explains:
After
mRNA vaccination the immune response against Spike is shifting to IgG4,
which is how your body responds after repeat exposure to stuff it needs
to tolerate, like bee venom, pollen or peanut proteins.
Our immune systems are complicated. We do need to fight dangerous replicating pathogens, such as viruses or bacteria. At the same time, we also face harmless inert substances, such as tree pollen, that sometimes cause inflammatory reactions called allergies.
To deal with these harmless substances, our immune system has a particular class of antibodies, called IgG4, that do the opposite of what we are used to hearing: they bind to allergens and tell our immune cells to ignore them rather than cause inflammation.
I had many pollen allergies. Every spring was unpleasant. I decided to go to an allergist and take allergy shots, which amounted to repeatedly injecting allergens into me. As a result of these repeat antigen shots, my immune system developed non-inflammatory IgG4 antibodies,
which mark pollen as a harmless substance to the rest of my immune
system and prevent allergic inflammation and nasty symptoms.
There is something important, though: pollen does not replicate.
It is a good idea not to have inflammation in response to pollen. It is a bad idea, however, to train our immune system to ignore replicating pathogens such as Sars-Cov-2.
How
would “immune tolerance,” induced by repeat antigen shots such as mRNA
injections, look like when the person is infected with Sars-Cov-2?
It would look like a “mild” infection without a serious fever that would last much longer than necessary and cause organ damage.
The sufferer may say, for the first week, that they are thankful for
vaccines and boosters making their symptoms mild. Then they start
wondering why the infection is not going away.
Such tolerance may explain why boosted people are the slowest to clear Covid-19:
A
new study just came out: It looked at how long “culturable virus” (that
is, virus capable of infecting people) is present in Covid patients
after the first positive test. The authors literally cultured swabs of
patients, on various days past-diagnosis, and counted how many patients,
by vaccination status, are still carrying live, replication-competent …
6 months ago · 433 likes · 451 comments · Igor Chudov
So: IgG4 antibodies have the opposite effect to all other types of antibodies and make our immune system ignore the particular antigen they are trained to detect.
You
do not want to ignore a replicating virus — so the IgG4 antibody class
would be inappropriate for viruses. Pollen, however, is a perfect case
for IgG4 to prevent immune reaction and inflammation.
Now
that you know what IgG4 antibodies are, let’s follow Rintrah’s
explanation of the study findings. The scientists followed several
subjects who underwent repeated mRNA vaccinations and subsequent
infections and tracked the composition of their antibodies.
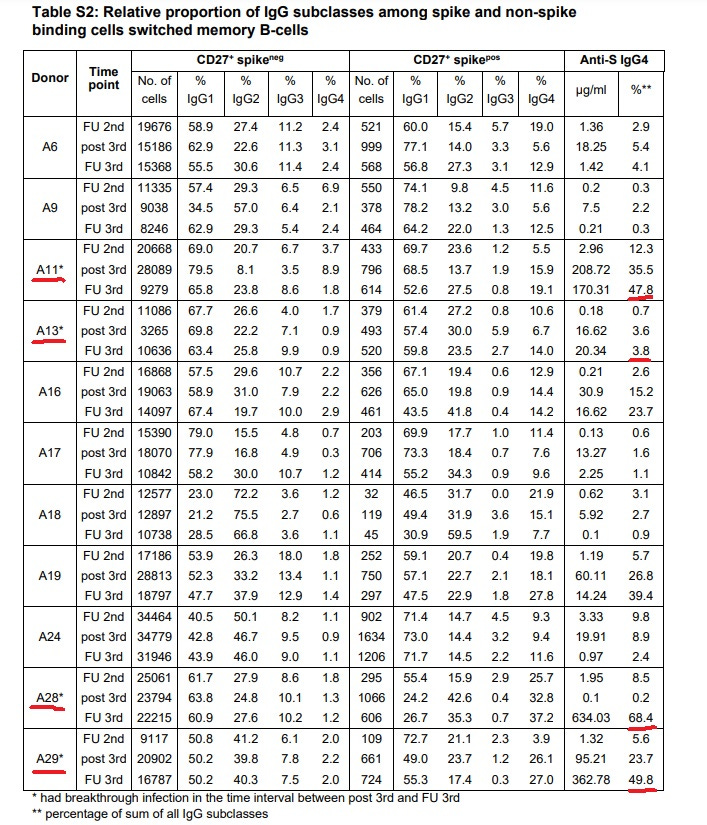
You
already know the story: After the second shot, IgG4 begins to show up.
This gets worse with the breakthrough infections, then it gets worse
again with the third shot. Now we have updated findings from breakthrough infections after the third shot. And this will shock you, but it gets worse again:
On
average, the four who had a breakthrough infection after their booster
are now at 42.45% IgG4. The cohort as a whole is at 19.27%, up from just
0.04%, so the ones who haven’t had a breakthrough
infection yet will end up at a similar position: A response that is
entirely IgG4 dominated.
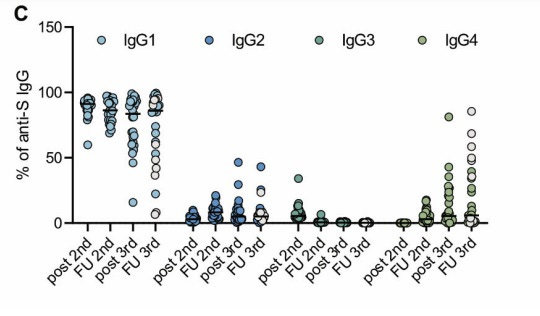
IgG4
isn’t really meant for neutralization. Out of the IgG’s, IgG3 is the
excellent virus neutralizer. What IgG3 does in the case of SARS2, is
that they have their tails bind together. This means that out of all the
four subclasses, IgG3 is showing 50-fold stronger neutralization than the other three subclasses against SARS2.
… Look at what happens to IgG3 after three shots:
There
is some IgG3 left in some people after the second shot, but by the time
they get the third shot, they’re all universally down to a flat zero.
So, Rintrah explains that the immunology study shows depletion of all-important, virus-fighting IgG3 antibodies and their replacement (class switch) with useless IgG4 antibodies. Those turn Covid infection to be needlessly “mild” but fail to clear the virus promptly.
We have fevers for a reason!
Again, if you have not read Rintrah’s article and have spare 30 minutes, take a look.
I mentioned immune tolerance last June, referring to a surprisingly lucid Internet prediction from Sep 2021 that was coming true epidemiologically:
In
the last section of my post from yesterday, I asked, why doesn’t
Paxlovid work for vaccinated people. Try to stop and think for a minute.
Ask yourself a question: why, exactly, is Paxlovid not working in the
vaccinated? The problem is not with Paxlovid, it is the same medication
as given to the unvaccinated. The problem is with the immune systems of
th…
6 months ago · 349 likes · 355 comments · Igor Chudov
The infamous substacker Brian Mowrey posted a great post last July. He introduces us to IgG4 and immune tolerance:
Spike-overload
finally seems to be showing a concrete effect in the repeat-injected: B
Cells in two separate cohorts were found to be self-switching to IgG4
class antibodies, associated with tolerance and anti-inflammatory
response, after the 3rd dose…
5 months ago · 97 likes · 64 comments · Brian Mowrey
I will mention a few of my related posts in the links below.
Immune tolerance prevents rapid clearance of the infection, making boosted people the slowest to clear Covid-19.
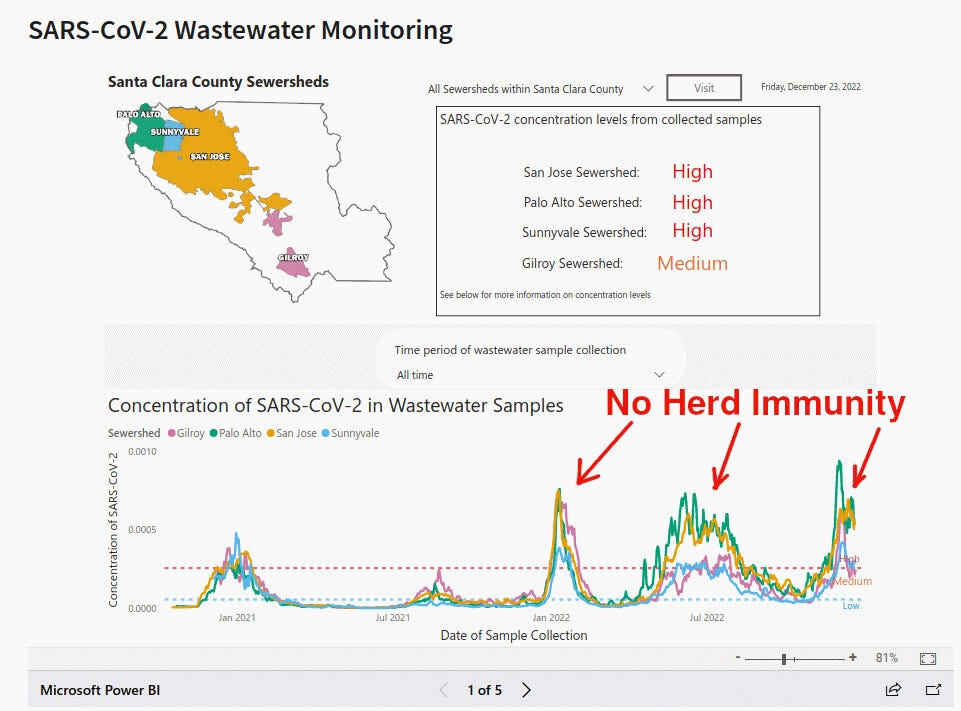
It prevents the formation of lasting neutralizing immunity, thus making affected people suffer from repeat reinfections. In other words, forget herd immunity.
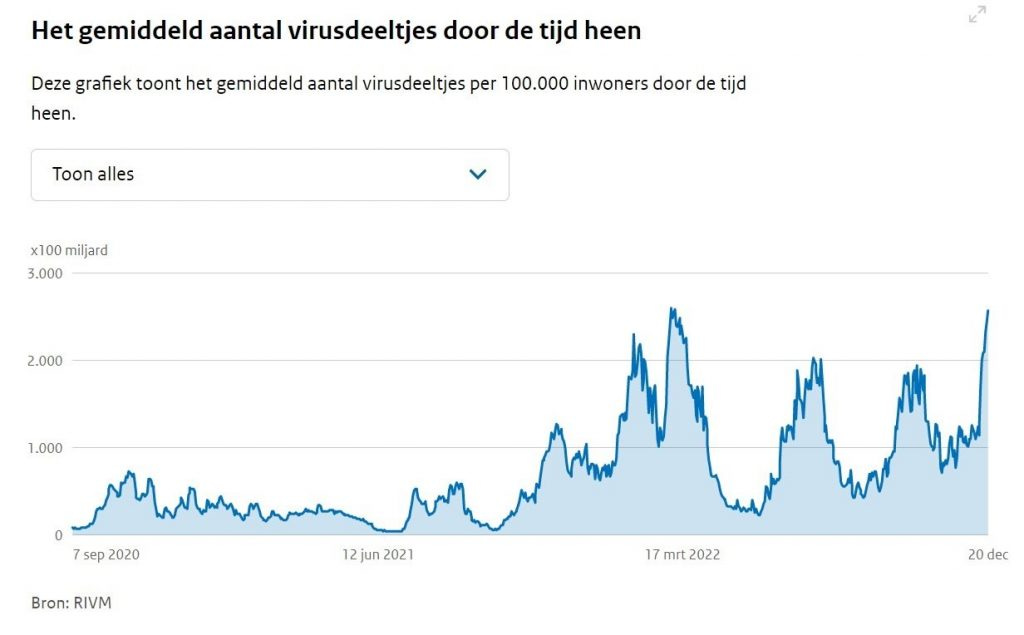
The utter absence of herd immunity can be seen in this Santa Clara County, California chart of Sars-Cov-2 in wastewater:
Rintrah shows the same type of picture for his highly-vaccinated motherland Netherlands:
Could repeat Covid infections, caused by immune tolerance, lead to increased mortality? Absolutely! This Singapore study
suggests that most excess deaths in Singapore happen within 90 days of a
Covid infection. A lot of such deaths, unfortunately, are not recorded
as Covid deaths. They could be recorded as “sudden deaths” from “unknown
cause.”
The disease may seem mild
if immune tolerance fails to elicit a strong reaction and stop viral
replication. The virus, proliferating unopposed, damages the
cardiovascular system more than in those who can
mount a vigorous immune reaction. One such victim is Gwen Casten, a
17-year-old daughter of vaccine-loving congressman Sean Casten. Gwen died suddenly in her sleep in June of 2022 after suffering a “very mild” Covid infection.
It takes time for immune tolerance to develop after boosting. As the Immunology article says:
These
three individuals experienced the infection with the largest time
difference to the last vaccination, at 95, 201 or 257 days after the
second vaccination, while in the other nine patients the infection took
place between 25 and 78 days after the second mRNA shot. This supports
the hypothesis that the switch to IgG4 is a consequence of ongoing GC maturation and that it takes several months until IgG4-switched memory B cells appear.
This “taking time to develop” is a biological time bomb placed into the immune systems of boosted people! It takes the germinal centers months after the third injection to switch to the useless IgG4.
Therefore,
many months after the booster dose, a Covid infection is met with
worthless, forgiving, and disease-ignoring IgG4 antibodies. The
infection seems mild; the virus replicates unopposed due to the IgG4
switch; the cardiovascular system is damaged; the risk of sudden death
multiplies!
A while ago, I asked: why does the strength of the statistical association between vaccines and excess deaths increase over time?
Immune tolerance developing MONTHS after booster shots perfectly explains the strange delayed effect seen in excess mortality - and why vaccination rates explain more and more excess deaths as time passes.
What have we done?
Perhaps we should not have conducted vaccine trials at Warp Speed?
What will happen to all of us if we cannot get herd immunity and many people develop dangerous immune tolerance?
Share