A
month ago, I mentioned evidence (provided by the Dutch Institute RIVM)
of a dramatic increase in cognitive problems among adults:
That
post struck a nerve and prompted many readers to share their
observations and feelings about cognitive changes they observed in
themselves or their loved ones. As of today, the post garnered 1,263 comments!
A friend of this blog, a popular substacker A Midwestern Doctor,
offered to share further thoughts and observations. As I consider this
to be a supremely important topic, I hope that the below text, which I
did not write, will promote further discussion and thinking about the
cognitive changes we observe.
I
know many vaccinated and many unvaccinated people. Many of them,
thankfully, are fine. Some have issues while remaining good, promising,
and valuable human beings. I hope the struggles of those with emergent
difficulties with the executive function will prompt a search for
solutions.
While
the thoughts below concentrate on vaccine-related issues, I plan on
exploring this topic in the future and looking into other factors that
may also affect human intellectual functioning.
The text below was written by A Midwestern Doctor.
I want to offer it as food for thought. As always, you are welcome to
agree or disagree with anything; your opinions will not be censored. So
comment away!
When
the COVID-19 vaccines were brought to market, due to their design I
expected them to have safety issues, and I expected over the long term, a
variety of chronic issues would be linked to them. This was because
there were a variety of reasons to suspect they would cause autoimmune
disorders, fertility issues and cancers—but for some reason (as shown by
the Pfizer EMA leaks), the vaccines had been exempted from being appropriately tested for any of these issues prior to being given to humans.
Since
all new drugs are required to receive that testing, I interpreted it to
be a tacit admission it was known major issues would emerge in these
areas, and that a decision was made that it was better to just not
officially test any of them so there would be no data to show Pfizer
knew the problems would develop. Sadly, since the time the vaccines
entered the market, those three issues (especially autoimmunity) have
become some of the most common severe events associated with the
vaccines.
At the start of the vaccine rollout, there were four red flags to me:
•The
early advertising campaigns for the vaccines mentioned that you would
feel awful when you got the vaccine, but that was fine and a sign the
vaccine was working. Even with vaccines that had a very high rate of
adverse events (e.g., the HPV vaccine),
I never saw this mentioned. This signified it was likely the adverse
event rate with the spike protein vaccines would be much higher than
normal.
•Many of my colleagues who got the vaccine
(since they were healthcare workers they were able to get it first)
posted on social media about just how awful they felt after getting the
vaccine. This was also something I had never seen with a previous
vaccine. After some digging, I noticed those with the worse vaccine
reactions typically had already had COVID and had their reaction was to
the second shot rather than the first, signifying that some type of
increased sensitization was occurring from repeated exposures to the
spike protein. Likewise, the published clinical trial about Pfizer’s vaccine also showed adverse reactions were much higher with the second rather than first shot.
•Once
it became available to the general public, I immediately had patients
start showing up with vaccine reactions, many of whom stated they
received their flu shot each year and never had experienced something
similar with a previous vaccination. One of the most concerning things
were the pre-exacerbation of autoimmune diseases (e.g., spots in their
body they previously would occasionally have arthritis in all felt like
they were on fire). After I started looking into this I realized people
were seeing between a 15-25% rate of new autoimmune disorders or
exacerbations of existing autoimmune disorders developing after the
vaccine (later shown in an Israeli survey), a massive increase I had never seen any previous vaccine cause.
•About
a month after the vaccines were available to the public, I started
having friends and patients share that they’d known someone who had
unexpectedly died suddenly after receiving the vaccine (typically from a
heart attack, stroke, or a sudden aggressive case of COVID-19).
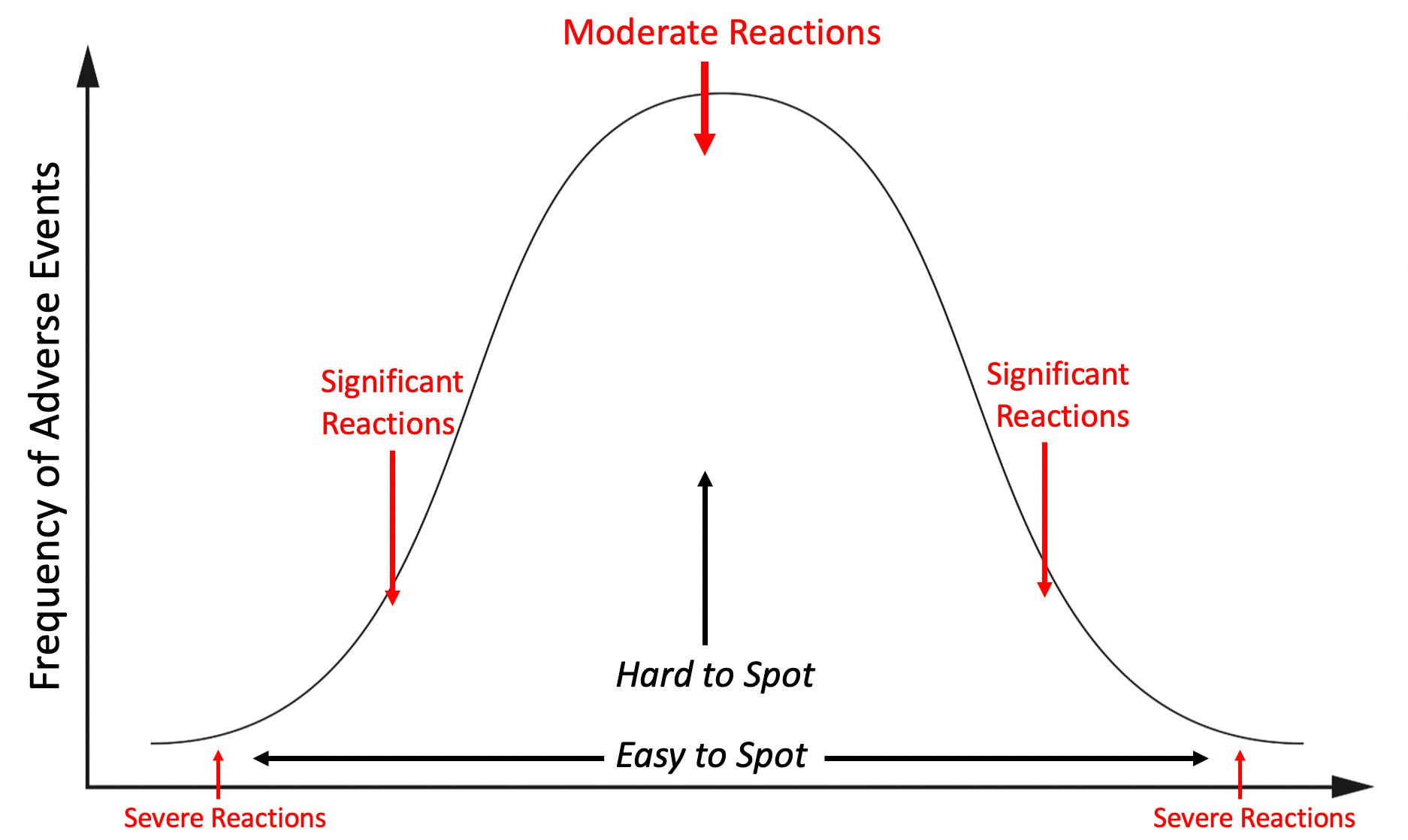
This
was extremely concerning to me, because reactions to a toxin typically
distribute on a bell curve, with the severe ones being much rarer than
the moderate ones. This meant that if that many severe reactions were
occurring, what I could already see was only the tip of the iceberg and
far, far more less obvious reactions were going to be happening, to the
point it was likely many people I knew would end up experiencing
complications from the vaccine.
I
tried to warn my colleagues about the dangers of this vaccine, but even
when I pointed out Pfizer’s own trial admitted the vaccine was more
likely to harm than help you, no one would listen to me. Not being sure
what else to do, but not be willing to do nothing, I decided to start documenting all the severe reactions I came across so I could have some type of “proof” to show my colleagues.
This
was something that was extremely important at the time since no one was
willing to take on the personal risk of publishing that something went
against the narrative (that vaccines were killing people) in the peer
reviewed literature. Shortly after Steve Kirsch kindly helped launched
my Substack, I decided to post the log I’d put together,
and since there was a critical need for that information, the post went
viral and created much of the initial reader base that made my substack
possible.
It
was immensely time consuming to do the project (especially the
verification of the story that was reported to me), so I ended the
project after a year. During that time,
I came across 45 cases of either a death (these compromised the
majority of the 45 cases), something I expected to be fatal later on
(e.g., a metastatic cancer) or a permanent complete disability.
Additionally, in line with the previously described bell curve, I also
came across many more significant but not as severe injuries.
I’ve
had a long term interest in studying pharmaceutical injuries because
many of my friends and relatives have had bad reactions to
pharmaceuticals. In most of these cases, ample data existed to show that
reaction could happen (often to the degree it strongly argued against
the pharmaceutical remaining on the market) and yet almost no one in the
medical field was aware of those dangers, hence leading to my injured
friends never being warned before they took the pharmaceutical or even
while the injury was occurring.
My
bell curve theory originally came about from examining all these cases.
I thus was interested to know exactly how the distribution of adverse
events from the spike protein vaccines would match what I had observed
with previous dangerous pharmaceuticals and if what I saw personally did
or did not match what everyone was reporting online.
One
of the things that immediately jumped out at me were the cases of a
friend’s parent in a nursing home receiving the vaccine, immediately
undergoing a rapid cognitive decline which was “diagnosed” as
Alzheimer’s disease and then dying not long after. At the time, I
assumed these were most likely due to undiagnosed ischemic strokes as
that was the most plausible mechanism to describe what I’d heard, but I
was not certain as I could never examine any of these individuals for
signs a stroke had indeed happened.
These
cases were very concerning to me, as they signified (per the bell
curve) that there was going to be a much larger portion of people who
would develop less severe (but nonetheless impactful) cognitive decline
following vaccination.
Note: one of the most
common types of injuries from pharmaceuticals are neurological injuries
which both impair cognitive function and create psychiatric symptoms.
This places patients in a difficult situation of being gaslighted
by the medical system. This is because their doctors assume the
psychiatric symptoms the patients are experiencing are the cause of
their illness rather than a symptom of it, leading to the patient being
told the illness is all in their head and continually referred for
psychiatric help. One of the best examples with this occurred as a
result of the abnormal heart rhythms (e.g., rapid anxiety provoking
palpitations) caused by the vaccine damaging the heart which were
consistently diagnosed as being a result of anxiety, even when a
subsequent workup I requested showed heart damage was present.
As
I began seeing more and more signs of cognitive impairment following
vaccination, I realized that what I observed mirrored what I previously
seen with chronic inflammatory conditions such as mold toxicity, HPV vaccine injuries, and lyme disease. Some of the examples included:
•Many
people reported having a “COVID” brain where it was just harder for
them to think and remember things. I saw this after more severe cases of
COVID, after vaccination, and in patients who per the time line
developed it from the vaccine but believed it had come from COVID.
•These
issues tended to be more likely to affect older adults, but younger
ones were more likely to notice (and complain) about them. In the case
of older adults, I typically learned about them from someone else who
had observed the cognitive decline rather than directly from the
individual.
•I saw cases of vaccine injured
individuals who had trouble remembering or recalling the word they knew
expressed what they were trying to communicate (this is also a common
mold toxicity symptom).
•I knew a few people (e.g.,
friends and colleagues) who told me their brain just didn’t work the
same since they’d received the vaccine.
•I saw cases
of coworkers demonstrating noticeable (and permanent) cognitive
impairment after I’d assumed they’d received the vaccine. Their
impairment was never mentioned or addressed (rather the physician kept
on working, did not perform as well, and in some cases retired).
•I
met significantly injured vaccine injured patients who told me one of
the primary symptoms was a loss of cognitive functioning they had taken
for granted throughout their life. In many cases following treatment of
their vaccine injury, their cognition also improved.
•One
of my friends (a very smart immunologist) developed complications from
the first two vaccines and based on their symptoms was able to describe
exactly which parts of their immune systems were becoming dysregulated.
Against my advice, they took a booster and reported they suffered a
significant cognitive impairment never experienced before in their
lifetime. I feel this case was important to share as it illustrates how
an exacerbation of a vaccine injury can also cause an exacerbation of
cognitive symptoms.
Note: I also saw significant cognitive impairment occur in individuals who were acutely ill from COVID-19.
At
the same time I was observing these effects, many rumors (e.g., this
one) were also swirling around online that the vaccines would cause
cognitive impairment and that we would witness a zombie apocalypse from
the vaccine injuries.
This never happened, but many observed a suspicion cognitive impairment was occurring. For example to quote Igor’s recent article:
I
own a small business and deal with many people and other small
businesses. Most provided reliable service, would remember appointments,
followed up on issues, and so on. I noticed that lately, some people have become less capable cognitively. They forget essential appointments, cannot concentrate, make crazy-stupid mistakes, and so on.
In
my own case, the most evident change I noticed was a worsening of
drivers around me and had a few near misses from impaired driving.
The
challenge with these situations is that it’s very hard to tell if
something is actually happening or your perception is simply a product
of confirmation bias. For this reason, while I was comfortable asserting
my belief the COVID-19 vaccines were causing the severe injuries on
either end of the bell curve, I avoided doing so for many of the less
impactful injuries in the middle where it was much more ambiguous if
what I was observing was “real” or simply my own biased perception of
the events around me. Because of this, amongst other things, I never
mentioned the changes in driving I observed.
Typically,
when we have situations like this, large bodies of data or scientific
studies are needed to tease out if a correlation is in fact occurring.
Unfortunately, since there are political repercussions for dissenting
from the dominant narrative, data which threatens tends not to be
published. This creates the challenging situation where those who are
looking for answers on a topic which challenges a vested interest have
to look quite carefully for clues on the subject (e.g., by dissecting
papers to see exactly what the data is actually showing).
Igor
periodically finds those, and after I saw the most recent one he
unearthed, I requested to write a guest post. To quote his discovery
from the Netherlands:
Primary
care data for January to March 2023 showed that adults visited their GP
more frequently for a number of symptoms compared to the same period in
2019. Memory and concentration problems were significantly more common
than last year and in the period before COVID-19. Where these symptoms
are concerned, the difference compared to 2019 is growing steadily in each quarter.
In
the first quarter of 2023, there was a 24% increase in GP [general
practioner] visits related to memory and concentration problems among
adults (age 25 years and older) compared to the same period in 2020.
This is evidenced by the latest quarterly research update from the GOR Network. The increase in memory and concentration problems of adults seems to be a longer-term effect of the coronavirus measures as well as SARS-CoV-2 infections.
More specifically they found:
•No increase was observed in adults under 25 years old.
•A 31% increase was observed in those 24-44 years old.
•A 40% increase was observed in those 45-74 years old.
•A 18% increase was observed in those over 75 years old.
Note:
previous rounds of this survey, in addition to the cognitive issues
described above, worsening mental health (e.g, anxiety, depression or
suicidal thoughts), sleep problems, tiredness, and cardiovascular issues
(e.g., shortness of breath, dizziness or heart palpitation) were also
observed to have significantly increased since 2019.
Typically,
patients, less than 75 years old are unlikely to visit their doctors
for cognitive issues. Taken in context with this data, it means there is
a stronger case that the (massive) increases in those under 75 were
caused by something that happened
after 2019. Additionally, since there were already a large number of
visits for cognitive impairment in the elderly, the lower percentage
increase is slightly misleading in quantifying the extent to which
everyone was affected. For example to quote the previous report:
Primary
care data showed that adults visited their GP somewhat more frequently
for sleep problems in October–December 2022 than in the same period in
2019. This was particularly striking in the oldest age group (75 years
and older).
All
of this data put health officials in a bit of an awkward situation
since publishing data demonstrating large scale cognitive impairment
directly undermines the narrative they previous had committed themselves
to. Nonetheless, the authors of the report were significantly more
candid than many other before them:
The
source of this increase in memory and concentration problems is
unclear. A possible explanation could be that COVID-19 measures caused accelerated cognitive decline among people who were starting to have problems with memory and concentration (66 years on average).
COVID-19
was of course cited as a potential cause (which, as discussed above can
sometimes cause long term cognitive impairment):
A supplementary explanation
could be that some of these people have long-term symptoms after
COVID-19. Various studies have shown that memory and concentration
problems are common in post-COVID symptoms. Other infectious diseases,
such as flu, can also cause these symptoms. However, recent studies
have shown that long-term memory and concentration problems are much
more common after COVID-19 than after flu. In addition, these symptoms
are more common in older age groups. The figures provided by GPs are
consistent with this expectation.
Fortunately,
the authors acknowledged that long COVID could not be the primary
explanation for what was occurring, and instead alluded to the elephant
in the room—the vaccines.
Note:
on VAERS, in the 23 years VAERS has operated, 2352 of the 3071 (76.6%)
reports of memory impairment following vaccination came from the
COVID-19 vaccines.
My
specific interest in studying spike protein vaccine toxicity arose
because I suspected I would see many similarities to other
pharmaceutical injuries I had observed previously and treatments that
had developed for those injuries could be used to treat COVID-19 vaccine
injuries. On Substack, I’ve tried to focus on explaining the areas that
I believe are the most important to understanding this, zeta-potential,
the cell danger response (CDR) and the treatments for Alzheimer’s
disease. Note: Each of these is interrelated with and often causes the others.
Zeta Potential: Zeta potential (explained in detail here)
governs if fluid in the body clumps together (e.g., forming a clot) or
remains dispersed and capable of freely flowing. Additionally, it also
influences if proteins will stay in their correct formation or misfold
and clump together. Many different issues (discussed here)
emerge when fluid circulation (be it blood, lymph, interstitial fluid
or cerebrospinal fluid) becomes impaired. Since the spike protein is
uniquely suited for impairing zeta potential, we have found restoring
zeta potential (discussed here)
often is immensely helpful during COVID-19 infections and for treating
COVID-19 vaccine injuries. Many of those approaches were initially
developed from working with other vaccine injuries and cognitive decline
in the elderly.
Cell Danger Response (CDR):
When cells are exposed to a threat, their mitochondria shift from
producing energy for the cell to a protective mode where the cell’s
metabolism and internal growth shuts down, the mitochondria release
reactive oxygen species to kill potential invaders, the cell warns other
cells to enter the CDR and the cell seals off and disconnects itself
from the body. The CDR (explained further here)
is an essential process for cellular survival, but frequently in
chronic illness, cells become stuck in it rather than allowing the
healing response to complete.
Understanding the CDR
is extremely important when working with complex illnesses because it
explains why triggers from long ago can cause an inexplicable illness,
and why many treatments that seem appropriate (specifically those that
treat a symptom of the CDR rather than the cause of it) either don’t
help or worsen the patient’s conditions. Many of the most challenging
patients seen by integrative practitioners are those trapped within the
CDR, but unfortunately, there is still very little knowledge of this
phenomena.
My interest was drawn back to the CDR after I realized that one of the most effective treatments
for long COVID and COVID-19 vaccine injuries was one that directly
treated the CDR. Since many of the therapies that have been developed to
revive nonfunctional tissue was developed by the regenerative medical
field, I wrote an article describing how these approaches are applied to
restore localized regions of dysfunctional tissue (which is sometimes
needed to treat vaccine injuries) and another on the regenerative
treatments that treat systemic CDRs (and are more frequently needed for vaccine injuries).
Alzheimer’s Disease (AD): AD is one of the most devastating and costly conditions in existence (e.g., for the year of 2020 it was estimated
to have cost America 305 billion dollars) and as a result, billions of
dollars are spent each year in researching a cure for it. This research (which began in 1906) has gone nowhere and presently the FDA is working with the drug industry to push forward ineffective, quite dangerous but highly profitable treatments for AD.
However, effective treatments do exist
for AD and my colleagues have developed a few different methods that
have successfully treated the condition. Additionally, one neurologist,
Dale Bresden developed a method for reversing AD that he proved worked in mulitiple publications (included a recent 2022 clinical trial).
All of these successful approaches utilize the following principles:
•Restore
both the blood flow to the brain and the lymphatic drainage from it
(which removes amyloid plaques). This often requires restoring the physiologic zeta potential and having healthy sleep cycle.
•Treating the CDR (which causes chronic inflammation) and reactivating brain cells that became trapped in an unresolved CDR (which amongst other things requires reclaiming a healthy sleep cycle).
Note: Bresden’s approach also emphasizes the importance of addressing chronically elevated blood sugar or insulin levels.
One
of the most important things to recognize about AD is that it is a
slowly worsening disease which often progresses over decades. In the
early stages of AD, minor cognitive changes occur, which (when possible
to autopsy) correlate with tissue changes within the brain. In rare
instances, individuals can instead have a rapidly progressing form of
Alzheimer's which strikes with a younger age and is often linked to the
toxin exposure.
In
the case of spike proteins illnesses, I have seen both the early signs
of AD cognitive decline occurring in much younger patients, and exist in
cases of AD rapidly progressing following vaccination.
Anytime
you attempt to perceive the world around you, you are always biased by
the pre-existing filters you have which prevent you from seeing much of
the world around you (discussed further here).
To some extent, these filters are a necessary evil as without them, the
world would be overwhelmingly complicated. However, if you cannot be
open to the possibility a biased filter this is clouding your perception
of reality, you become blind to a great deal of important things around
you. Misleading filters for example, explain why many of those
committed to the narrative cannot see the overwhelming evidence of
COVID-19 vaccine injuries around them.
One of the most commonly used filters is the "social proof,"
which essentially says people will typically not act on something,
believe it or even see it unless their peers (the herd) already are.
This creates a problem, because frequently when you need to know
something, the herd does not yet believe it, forcing you to either make a
decision no one else supports (which can be quite terrifying) or to
wait until there is safety in doing it because the herd has now moved in
that direction (which is often too late).
As
I’ve gotten to know those who challenged the COVID-19 narrative, I’ve
noticed they all had a tendency they’d learned through life experience
to not follow the crowd and be willing to act on their initial
impression of what preliminary data suggested before the rest of the
crowd caught on. For example, Ed Dowd was a highly successful stock
trader (e.g., he made Blackrock a lot of money) and his method boiled
down to spotting early trends before anyone else and acting on them.
Like
many, from the start of the vaccination campaign, based on the
preliminary data points that were available, I suspected it was going to
cause long-term cognitive issues. Now that the data which supports that
trend is beginning to appear, and concerningly the issue appears to be
gradually worsening, something commonly observed over time with factors
that give rise to dementia. This is an important issue and I want to
extend my thanks to Igor for drawing attention to this very important
dataset.
Share